Crime Prevention - Research Highlights 2017-H02-CP - Community Readiness and Mobilization

Background
In the United States and Canada, community readiness and mobilization strategies have been increasingly adopted by communities since the mid-1990s to address social issues, prevent crime, and improve cohesiveness among citizens. These pro-active and adaptable models allow the community and its members to identify the criminal, social or even health issues impacting them, and devise a plan to address problems on a broad level.Footnote1 Such strategies also allow unique populations, including Indigenous communities, to tailor interventions to their particular needs, such as cultural and traditional learning.Footnote2
Public Safety Canada provides national leadership in crime prevention by developing and disseminating practical knowledge on cost-effective programs and practices which address known risk and protective factors. The following research highlights provide guidelines that are complementary to the federal role of knowledge dissemination. By strengthening community readiness and mobilization, crime prevention efforts are strengthened. Furthermore, assessing community readiness and engaging partners are central steps at the pre-implementation phaseFootnote3. A well-planned and defined pre-implementation phase increases the probability of adequate program rollout as well as the chance of achieving the desired positive outcomes for participants.Footnote4
Community Readiness
What is it?
Community readiness can be defined as the “degree to which a community is willing and prepared to take action on an issue”.Footnote5 In other words, community readiness is a determination of how prepared a community is to deal with an issue concerning them, and how they can create positive change.Footnote6 A community’s readiness level is measured using comprehensive community readiness tools, and is then categorized in one of the nine different stages of readiness (Appendix A), from which specific strategies can be used to increase readiness and build towards community change.
Who can benefit from community readiness?
All communities facing challenges can benefit from community readiness. Assessing community readiness allows for an understanding of the specific needs and readiness of a community, which in turn sets the stage for intervention of their specific issue.Footnote7 Positive change can, therefore, be tailored to any issue, in any community, and assessed at an appropriate pace.
How do you assess community readiness?
Community readiness is assessed using comprehensive tools. Community readiness tools are survey-based instruments used to measure the awareness of an issue within a community in order to determine its stage of readiness. There are several different tools and interpretations available online to those seeking change in their community (Appendix B). The general steps to a community readiness assessment (that is, steps universal to most community readiness models) include the following:Footnote8
- Key stakeholders are asked to identify and define the community (e.g., by geographic location, organization, ethnic or occupational group, etc.) and the specific issue (such as substance abuse issues or suicide).
- Thorough interviews with respondents take place in the community. Interviews are used to collect information from a wide range of people (i.e., community leaders, professionals, and residents) with firsthand knowledge.
- Interview transcripts are then analyzed and scored to determine the level (or stage) of readiness of the community.Footnote9
- Strategies or action plans should then be developed by community representativesFootnote10 to help them achieve higher stages of readiness (see Appendix A for strategies to increase readiness).
Who should be involved in the community readiness assessment?
Community readiness assessments can be administered by anyone interested in community or social change. However, there are certain groups that either have firsthand knowledge of the issue or the resources and capacity to create change, which can result in increased chances for success. Examples of these groups include:
- Policymakers and planners;
- Community activists;
- Health and human services organizations; and
- Coalitions.Footnote11
Who should be surveyed in the community readiness assessment?
The population surveyed should depend on the specific issue affecting the community. For example, if the social issue is teen dating violence, adolescents should be among the primary groups consulted. Groups that could be consulted for an assessment include:
- Schools/Universities
- Municipal government
- Law enforcement
- Health & medical professions
- Social services
- Community at largeFootnote12
Why is it important to determine community readiness?
- It is cost effective in that it leverages available resources and partnerships to complete the process;
- Given the strong focus on community ownership, community readiness assessments help to ensure that strategies are based on the needs of the community, are culturally appropriate, and sustainable; and
- The process can be inexpensive, easy to use, and does not require professional expertise to administer.Footnote13
When should community readiness be measured?
Although the simplicity and low cost of community readiness assessments allow them to be administered at any time, there are certain situations where an assessment can be particularly useful. Such situations can include:
- Planning to deal with an emerging issue;
- Ongoing social change initiatives;
- Planning efforts involve community participation; or
- When multiple groups or communities are involved.Footnote14
It is important that the time for assessing community readiness and creating positive change come from within the community. Imposing solutions from the outside will not have the sustainable impact that positive change and readiness from within the community can achieve. The latter approach ensures community buy-in, better understanding of the issue at hand, and a tailored intervention to the needs of the community. Therefore, although outside support is sometimes necessary, the best time to determine community readiness is when the community itself is prepared for change.
Community Mobilization
What is it?
Once communities are ready to address a particular issue, mobilization can then take place. Community mobilization is a capacity building process through which individuals, groups, and organizations come together to address particular concerns within a given community, including issues associated with health and safety, crime prevention, and community development.Footnote15 Community mobilization emphasizes the importance of empowerment-based interventions to strengthen the norms and problem-solving resources of the community. Mobilization processes are more likely to succeed when they are based on complete information about the community, including:
- Information on the issues, problems, and concerns of the community;
- The community’s formal and informal strengths and assets;
- The community’s history addressing the issues;
- The power dynamics within the community; and
- The community’s knowledge and use of networks and resources outside the community.Footnote16
Community mobilization is approached using one of two models: a top-down approach of addressing needs conducted by external organizations, and a community empowerment approach focused on transforming the community from within. The following sections will cover the community empowerment model.
Who can benefit from community mobilization?
Like community readiness, any community needing to address an issue can benefit from the problem solving potential of community mobilization. Community-oriented programs and solutions that come from the mobilization process incorporate the concerns from community members and associated organizations, ensuring that the best approach is taken to address the problem of the community.Footnote17
When should community mobilization begin?
Community mobilization can begin when the community is ready to address a particular issue. The mobilization process usually begins with identifying and assessing the targeted issue, and setting priorities for development initiatives according to an action plan. The mobilization process should follow a readiness assessment.
How do we engage in community mobilization?
Since communities are not homogenous, mobilization efforts cannot be standardized. Rather, mobilization efforts must be sensitive to the specific context, motivation, and level of readiness of each community.Footnote18 Despite such considerations, research has identified common features that a number of mobilization efforts tend to encompass:
- Communities should develop collaborative partnershipsFootnote19 from multiple sectors before engaging in mobilization practices.
- Decisions or clarifications related to partners’ and leaders’ roles should be formalized in a written agreement.
- A certain level of capacityFootnote20 is also necessary for effective community mobilization.
- Community members must ensure that performance measures, such as community surveys and cost-benefit analyses, are in place to determine the effectiveness of their mobilization practices.
- Communities must ensure that resource attribution is tailored to their particular circumstances.
- Communities must also consider the short and long-term goals and create realistic expectations prior to starting mobilization efforts.Footnote21
The 5 stages of the Community Mobilization Framework
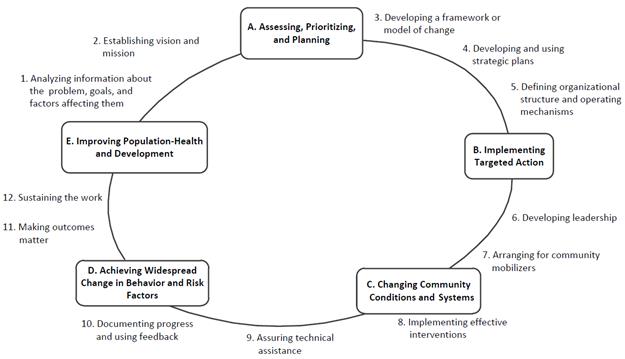
Image description\
The basic process of community mobilization is divided into several steps, and is illustrated using the Community Mobilization Framework.Footnote22 According to Watson-Thompson et al. (2008), there are five stages to this framework: (A) Assessing, Prioritizing, and Planning; (B) Implementing Targeted Action; (C) Changing Community Conditions and Systems; (D) Achieving Change in Behaviour and Risk Factors; and (E) Improving Population-Health and Development.
(From Watson-Thompson et al., 2008)
- (A) Assessing, Prioritizing, and Planning – During this stage, representatives from the private and public sector come together to share resources and responsibilities to address community concerns. This stage of the framework covers the concept of community readiness and covers activities 1 to 5 of the above illustration.
- (B) Implementing Targeted Action – Developing leadership is a vital process within this stage, because it provides community partners and stakeholders with the individual and collective capacity to mobilize for change and improvement. Community mobilizers are recruited in order to ensure support for systematic implementation of the strategic plan and the facilitation of community change. This stage covers activities 6 and 7.
- (C) Changing Community Conditions and Systems – This stage typically requires the implementation of effective interventions that are adapted to specific community contexts, conditions, and needs. To do this, community members must provide technical assistance and other resources. Within this stage, progress must be documented and feedback must be provided to all individuals involved. This stage covers activities 8 to 10.
- (D) Change in Behaviour and Risk Factors - Change efforts are outcome-oriented; they aim to reduce negative outcomes and promote positive development. Improving population-level outcomes, however, requires widespread change in the thoughts and behaviours of multiple actors. Sustaining the work is also a critical component to ensure the continued viability of community mobilization efforts by leveraging ongoing human, financial, organizational, and community resources. This stage covers activities 11 and 12.
- (E) Improving Population-Health and Development - Community mobilization efforts best promote healthy development when training and specific opportunities are made available, especially to youth. Training youth and other leaders to be mobilizers within the community provides a complementary voice for positive change.
Who should be involved in community mobilization?
Community mobilization is a communal effort and focuses largely on the use of local expertise. Mobilization begins with community leaders (e.g. concerned community members, invested organizations) who help facilitate the capacity building process and promote community expertise and participation. Important stakeholders included in the decision making process for community mobilization can include local governments, police, businesses, and community members, including youth.Footnote23
Why use community mobilization for change?
- It allows for the participation of volunteers, community members, and community organizations who might not normally have a voice in change.
- It allows the community to create local solutions to local problems; the mobilization approach can be culturally appropriate and satisfy specific needs of the community.
- Community mobilization surpasses intervention; it creates change from within that will last well beyond the implementation of external-type projects.
- Community ownership of the problem allows for an expanded base of support.
- It fosters strong relationships between local governments, businesses and community members.Footnote24
Readiness and mobilization in Indigenous communities
Public Safety Canada and community mobilization
In 2009, Public Safety Canada’s Aboriginal Corrections Policy Unit held the Semaganis Gatherings in six provinces/territories across Canada. The purpose of these gatherings was to establish a dialogue between First Nations (Ojibwe, Mi’kmaq, Dene, Blackfoot, and Kwakitutl) and urban Indigenous groups about community mobilization practices (Public Safety Canada, 2009).
From these gatherings, common themes emerged about how mobilization should be approached and implemented within Indigenous communities. During these discussions, it was acknowledged that mobilization processes can be culturally appropriate and more meaningful to the community if they are based on the First Nation Principles of OCAP (ownership, control, access, and possession). These principles allow Indigenous communities to control the information collected from their communities and enables them to make decisions on how it is eventually used to help the community mobilize.Footnote25 Other conclusions from the gatherings include:
- Mobilization practices should be locally driven and must involve local expertise and local community members in order to be successful;
- Elders should work in collaboration with youth so that they feel invested in their communities; and
- Those engaged in community mobilization practices should possess a number of skills in order to meet the needs of Indigenous communities, such as knowledge of cultural traditions, the ability to speak the cultural language, and the ability to motivate others through effective communication.
The Aboriginal Community Safety Planning Initiative
The Aboriginal Community Safety Planning Initiative (ACSPI) was created in 2010 as part of the Canadian government’s concrete action to address the disturbingly high number of missing and murdered Indigenous women. The goal of this initiative is to support communities in identifying risks and social issues within it (community readiness), and aid them in developing resource-friendly Community Safety Plans (CSPs) to address identified risks and social issues (community mobilization). The process of the ACSPI is very much community-oriented, as trained facilitators from Public Safety (PS) work in collaboration with core members of the community to develop a CSP with a great emphasis on leadership, ownership, community identity, and strategic vision.Footnote26
Results
To date, as part of the ACSPI, 25 CSPs have been completed with Indigenous communities across Canada, with an additional 10 more CSPs planned. Of the evaluated CSPs, a large number of communities (11) have significantly advanced their mobilization and safety planning process; 6 communities have shown positive, but limited progress to their mobilization process; and eight communities have shown little engagement to safety planning and mobilization. Evaluation results indicated improved outcomes, including awareness of community issues and community motivation to address issues.Footnote27 However, challenges to engagement were also identified in the results. Such challenges included sustainability, lack of initial clarity about the initiative’s goals, and lack of buy-in from administrators.Footnote28
Program example
The Peepeekisis project, which addressed the issue of spousal abuse, is an example of a community mobilization approach yielding positive responses. The project included a 52 week training program for community elders focusing on healthy relationships, addictions, and anger management. The support group portion of the project met regularly and included couples from various age groups and status, including individuals currently on parole. The project was viewed by stakeholders as a highly successful initiative, extending well beyond the project’s initial scope; from an implementation standpoint, the project remains a model on which to base future programs.Footnote29
Conclusion
In terms of addressing social issues among at-risk populations, community readiness and mobilization strategies have historically been successful in both theory and practice. However, simply understanding the different models of readiness and mobilization, as well as their respective strengths and limitations, is not enough; it is essential to acknowledge the importance of the community, not only as the stage of intervention, but as an active player in the healing process. As the Community Safety Plan evaluations have demonstrated, the level of community investment in the developmental initiative has been identified as a key indicator in determining success.Footnote30 Community readiness and mobilization strategies have also been successfully implemented in different countriesFootnote31 and disciplinesFootnote32, increasing the knowledge base of how readiness and mobilization practices can help communities address both emerging and persistent issues.
Appendix A
The following table represents the nine stages of community readiness, as well as strategies that can be used to increase the level of readiness within communities. Although these stages can be used to assess the readiness of a community towards any social issue, the example of substance abuse is illustrated below.
Readiness Stage |
Brief Description |
Strategies to Increase ReadinessFootnote34 |
|---|---|---|
1.Community Tolerance / No Knowledge |
Substance abuse is generally not recognized by the community or leaders as a problem. “It’s just the way things are” is a common attitude. Community norms may encourage or tolerate the behaviour in social context. Substance abuse may be attributed to certain age, sex, racial, or class groups. |
|
2. Denial |
There is little or no recognition that substance abuse is a community problem. Attitudes may include “It’s not my problem” or “We can’t do anything about it.” |
|
3.Vague Awareness |
There is a general feeling among some in the community that there is a problem and that something ought to be done, but motivation is lacking. Knowledge about the problem is limited. No identifiable leadership exists, or leadership is not encouraged. |
|
4. Pre-planning |
There is clear recognition by many that there is a local problem and something needs to be done. There is general information about local problems and some discussion. There may be leaders and a committee to address the problem, but no real planning or clear idea of how to progress has been formed. |
|
5. Preparation |
The community has begun planning and is focused on practical details. There is general information about local problems and about the pros and cons of prevention programs, but data is lacking. Leadership is active and energetic. Decisions are being made and resources (time, money, people, etc.) are being sought and allocated. |
|
6. Initiation |
Data is collected to justify a prevention program. At this stage, decisions may still be based on generalities rather than the new data collected. This stage usually marks the beginning of action being taken and staff being trained. |
|
7. Institutionalization & Stabilization |
Several planned efforts are underway and supported by community decision makers. Programs and activities are seen as stable, and staff is trained and experienced. Action is supported by most of the community, but not all. Evaluation may be limited, although some data is routinely gathered. |
|
8. Confirmation & Expansion |
Efforts and activities are in place, and community members are participating. Programs have been evaluated and modified, if necessary. Leaders support expanding funding and program scope. Data is regularly collected and used to drive programming. |
|
9. Professionalization |
The community has detailed, sophisticated knowledge of prevalence and risk and protective factors. Primary, secondary and tertiary efforts are in place for a variety of populations. Staff is well trained and experienced. Effective evaluation is routine and used to modify activities. Community involvement is high. |
|
Appendix B
The following table includes examples of tools and models to assess community readiness. The following list is not exhaustive, but represents key tools used in North America and their main components.
Tool |
Dimensions Covered |
From Whom Is Data Collected? |
Key Elements |
Instrument Considerations |
|---|---|---|---|---|
Assessing Community Readiness & Implementing Risk Reduction Strategies – Manual Source: The Canadian Aboriginal AIDS Network (CAAN) For more information: |
|
|
|
|
Community Key Leader Survey Source: Goodman and Wandersman For more information: |
|
|
|
|
Community Prevention Readiness Index Source: Community Partner Institute For more information: |
|
|
|
|
Community Readiness Model (CRM) Source: Tri-Ethnic Center For more information: |
|
|
|
|
Community Readiness Survey Source: Minnesota Institute of Public Health For more information: Beebe, T. J., Harrison, P. A., Sharma, A., & Hedger, S. (2001). The Community Readiness Survey: Development and initial validation. Evaluation Review, 25, 55-71. |
|
|
|
|
References
Advocates for Youth. (2008). Strategies Guided by Best Practice for Community Mobilization. Retrieved from: http://www.advocatesforyouth.org/publications/publications-a-z/2398-strategies-guided-by-best-practice-for-community-mobilization.
Calliou, B., & Wesley-Esquimaux, C. (2014). Wise practices approach to indigenous community development in Canada. In C. J. Voyager, L. Brearly, B. Calliou (Eds.), Restorying indigenous leadership: Wise practices in community development (pp. 31-60). Alberta, CA: Banff Centre Press.
Canadian Aboriginal AIDS Network. (2016). Assessing Community Readiness & Implementing Risk Reduction Strategies: Manual. Retrieved from: http://caan.ca/wp-content/uploads/2012/05/CR-manual-eng.pdf.
Community Tool Box. (2016). Community Readiness. Other Models for Promoting Community Health and Development. Chapter 2. Section 9. Retrieved 28 February 2017, from http://ctb.ku.edu/en/table-of-contents/overview/models-for-community-health-and-development/community-readiness/main.
Feathers, P. (n.d.). Comparison of Community Readiness Assessment Tools. Southwest Center for Applied Prevention Technologies. Retrieved from: http://www.drugs.indiana.edu/spf/docs/Comparison%20of%20Community%20Readiness%20Assessment%20Tools.pdf.
First Nations Information Governance Centre (FNIGC). (2017). The First Nations Principles of OCAP®. Retrieved from: http://fnigc.ca/ocap.html.
Fixsen, D., Naoom, S., Blase, K., Friedman, R., Wallace, F. (2005). Implementation Research: A Synthesis of the Literature. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, National Implementation Research Network.
Fletcher, F., Hibbert, A., Robertson, F., & Asselin, J. (2013). Needs and readiness assessments: Tools for promoting community-university engagement with Aboriginal communities. Gateways: International Journal of Community Research and Engagement, 6(1), 131-49.
Florida Department of Health. (n.d.). Community Mobilization. Retrieved 1 March 2017, from https://www.myctb.org/wst/floridacommunityprevention/mobilization/default.aspx.
Green, G. P. (2010). Community assets: Building the capacity for development. In G. P. Green & A. Goetting (Eds.), Mobilizing communities: Asset building as a community development strategy (pp. 1-13). Philadelphia, PA: Temple University Press.
Hastings, R., & Jamieson, W. (2002). Community Mobilization and Crime Prevention. Report to the National Crime Prevention Centre, Department of Justice Canada.
Jamieson, W. (2008). Factors related to successful mobilization of communities for crime prevention. IPC Review, 2, 11-33.
Jumper-Thurman, P., Plested, B. A., Edwards, R. W., Foley, R., & Burnside, M. (2003). Community readiness: The journey to community healing. Journal of Psychoactive Drugs, 35(1), 27-31.
Jumper-Thurman, P., & Plested, B. A. (2000). Community readiness: A model for healing in a rural Alaskan community. The Family Psychologist,(Summer), 8-9.
Kretzmann, J. P., & Mcknight, J. L. (1993). Building communities from the inside out. ACTA Publications: Chicago, Illinois.
Plested, B. A., Jumper-Thurman, P., & Edwards, R. W. (2014). Community Readiness Manual on Suicide Prevention in Native Communities. Retrieved from: http://www.samhsa.gov/sites/default/files/tribal_tta_center_2.3.b_commreadinessmanual_final_3.6.14.pdf.
Public Safety Canada. (2016). Aboriginal Community Safety Planning & Collaborative Implementation. (Unpublished presentation).
Public Safety Canada. (2014). 2013-2014 Evaluation of the Aboriginal Community Safety Development Contribution Program: Final Report.
Public Safety Canada. (2009). Community Mobilisation Dialogue with Aboriginal Communities, Aboriginal Corrections Policy Unit. Retrieved from: https://www.publicsafety.gc.ca/cnt/rsrcs/pblctns/cmmnt-mblstn/index-en.aspx.
Substance Abuse and Mental Health Services Administration's Center for the Application of Prevention Technologies. (2016). Tools to Assess Community Readiness to Prevent Substance Misuse. Retrieved from: https://www.samhsa.gov/capt/sites/default/files/resources/community-readiness-tools.pdf.
Sanchez-Way, R., & Johnson, S. (2000). Cultural practices in American Indian prevention programs. Retrieved from: https://www.ncjrs.gov/html/ojjdp/jjnl_2000_12/cult.html.
Status of Women Canada. (2016). Project Examples - Action Plan to Address Family Violence and Violent Crimes Against Aboriginal Women and Girls - Status of Women Canada. Retrieved from: http://www.swc-cfc.gc.ca/fun-fin/ap-pa/proj-en.html.
Transforming Communities. (1999). Benefits and Challenges of Community Mobilization for Domestic Violence Programs. Learning and Training Institute Manual.
Tri-Ethnic Center for Prevention Research. (2014). Community Readiness for Community Change: The Tri-Ethnic Center Community Readiness Handbook (2nd Edition). Colorado State University. Retrieved from: http://triethniccenter.colostate.edu/docs/CR_Handbook_8-3-15.pdf
Watson-Thompson, J., Fawcett, S. B., & Schultz, J. A. (2008). A framework for community mobilization to promote healthy youth development. American Journal of Preventive Medicine, 34(3), 72-80.
Wesley-Esquimaux, C., & Calliou, B. (2010). Best Practices in Aboriginal Community Development: A Literature Review and Wise Practices Approach, the Banff Centre. Retrieved from: http://fnbc.info/sites/default/files/resource-files/best_practices_in_aboriginal_community_development.pdf
For more information on research at the Community Safety and Countering Crime Branch, Public Safety Canada, or to be placed on our distribution list, please contact:
Research Division Public Safety Canada 340 Laurier Avenue West Ottawa, Ontario K1A 0P8 PS.CPBResearch-RechercheSPC.SP@ps-sp.gc.ca
Research Highlights are produced for the Community Safety and Countering Crime Branch, Public Safety Canada. The summary herein reflects interpretations of the report authors' findings and do not necessarily reflect those of the Department of Public Safety Canada. ISSN: 2560-7723
Footnotes
- 1
Kretzmann & Mcknight, 1993; Plested et al. 2014; Tri-Ethnic Center for Prevention Research, 2014
- 2
CAAN, 2016; Sanchez-Way & Johnson, 2000; Calliou & Wesley-Esquimaux, 2014
- 3
According to the National Implementation Research Network (NIRN), the implementation process is divided into four stages: exploration (which includes community assessment), installation, initial implementation and full implementation. For more information, consult Fixsen et al., 2005
- 4
The National Implementation Research Network’s website available at: http://nirn.fpg.unc.edu/. For more information, also consult: Saldana, Chamberlain, Wang, & Brown, 2011; Slavin, Madden, Chamberlain, & Cheung, 2010
- 5
Tri-Ethnic Center for Prevention Research, 2014, p. 4
- 6
Community Tool Box, 2016. For more information on Community readiness and development, please visit http://ctb.ku.edu/en/table-of-contents/overview/models-for-community-health-and-development/community-readiness/main.
- 7
Community Tool Box, 2016
- 8
Feathers, n.d.; Tri-Ethnic Center for Prevention Research, 2014
- 9
Certain community readiness initiatives also score the community readiness based on dimensions. Using the same 9 stages of readiness, these programs can determine the level of leadership, networking, existing prevention methods, and capacity (and more) within their community, along with their general stage of readiness. Community readiness programs are not restricted to only one dimension. See Appendix B for the dimensions used in different tools.
- 10
Core members of the community invested/participating in the community readiness process
- 11
Community Tool Box, 2016
- 12
Community Tool Box, 2016
- 13
Community Tool Box, 2016
- 14
Community Tool Box, 2016
- 15
Advocates for Youth, 2008; Hastings & Jamieson, 2002
- 16
Hastings & Jamieson, 2002
- 17
Florida Department of Health, n.d.
- 18
Jamieson, 2008
- 19
“Collaborative relationships” are characterized by a commitment to mutual goals; a jointly developed structure and shared responsibility; mutual authority and accountability for success; and the sharing of resources and rewards.
- 20
“Community capacity”, defined as a community’s collective ability to undertake collective action Green, 2010; Jamieson, 2008; Hastings & Jamieson, 2002, is related to many aspects, including:
- Economic capital, i.e. financial resources accessed from external sources
- Physical capital, i.e. the infrastructure and equipment of the community, such as housing, roads, utilities
- Human capital, i.e. the skills, knowledge, attitudes, and understanding of people in the community
- Social capital, i.e. (the breadth and depth of social relationships in the community
- Spiritual/cultural capital, i.e. values, symbols, traditions, and language of the community
- Political capital, i.e. forms of governance, inclusive systems of decision making
- Environmental capital, i.e. the natural resources of the community.
- 21
Green, 2010; Jamieson, 2008
- 22
Watson-Thompson et al. 2008
- 23
Florida Department of Health, n.d; Hastings & Jamieson, 2002
- 24
Transforming Communities, 1999; Florida Department of Health, n.d.
- 25
Public Safety Canada, 2009
- 26
Public Safety Canada, 2016. For more information on the Aboriginal Community Safety Planning Initiative, please visit https://www.publicsafety.gc.ca/cnt/cntrng-crm/crrctns/cmmnt-sft-cntrbtn-prgrm-en.aspx.
- 27
Public Safety Canada, 2014
- 28
Public Safety Canada, 2014
- 29
Public Safety Canada, 2014; Status of Women Canada, 2016
- 30
Public Safety Canada, 2014
- 31
There is evidence supporting community readiness and mobilizations’ ability to help indigenous communities in the United States, as certain tools have already been used in small Alaskan communities to deal with pressing social problems, such as alcoholism and suicide.
- 32
The Canadian Aboriginal Aids Network’s (CAAN) adaptation of the Community Readiness Model from the Tri-Ethnic Prevention Center was used to help Aboriginal communities dealing with HIV/AIDS issues, by assessing the community readiness and implementing risk reduction practices (CAAN, 2016).
- 33
Feathers, n.d.
- 34
Points to consider when developing strategies to achieve higher stages of readiness:
- Consider who is being targeted so that the message is formulated appropriately and delivered to the right audience.
- The message should reflect the goals that have been set in the strategy and leave a lasting impression on the target audience. Emotional or moral appeals and personal stories are effective measures to gain the attention of the target audience.
- Chosen community representatives should influence the audience and act as an important role model.
- Social networks should be identified in accordance with particular goals and could be arranged by sectors (i.e., health), interests (i.e., hobby groups), age (i.e., elders), or ethnicity. (Tri-Ethnic Center for Prevention Research, 2014)
- 35
SAMHSA's Center for the Application of Prevention Technologies, 2016
- Date modified: